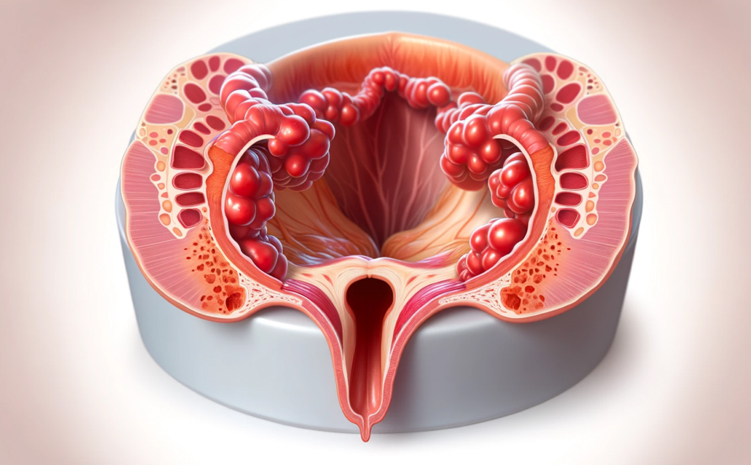
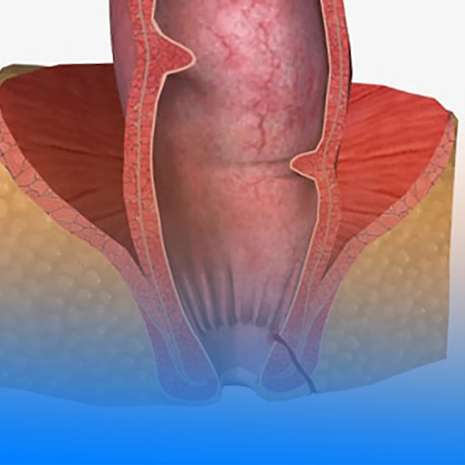
Anismus is a functional defecation disorder in which the pelvic floor muscles and anal sphincter fail to relax, or paradoxically contract, during bowel movements. Although there is no structural blockage in the intestines, this abnormal muscle coordination makes stool evacuation difficult. Patients often experience excessive straining, prolonged time on the toilet, a sensation of incomplete evacuation, and sometimes the need for digital assistance. Anismus is commonly associated with chronic constipation and may persist for years without proper diagnosis and treatment.
What is anismus?
Anismus is a functional defecation disorder in which the pelvic floor muscles and anal sphincter fail to relax, or paradoxically contract, during bowel movements. Although there is no structural obstruction in the intestines, improper muscle coordination prevents normal stool evacuation. Patients commonly experience prolonged time on the toilet, excessive straining, a sensation of incomplete evacuation, and sometimes the need for digital assistance. Anismus is frequently associated with chronic constipation and may persist for years if not properly diagnosed.
What are the symptoms of anismus?
Symptoms of anismus are mainly related to bowel movements and often become chronic over time. Common complaints include excessive straining, a sensation of incomplete bowel emptying, prolonged time spent on the toilet, hard stools, bloating and gas. Some patients experience a feeling of blockage in the anal area and may need digital assistance to evacuate stool. Anismus is frequently associated with chronic constipation and can significantly impair quality of life if left untreated.
How is anismus diagnosed?
Anismus is diagnosed by carefully evaluating the patient’s symptoms and performing a detailed proctological examination. During digital rectal examination, the patient is asked to strain in order to assess coordination of the pelvic floor and anal muscles. To confirm the diagnosis, functional tests such as anorectal manometry, balloon expulsion test, and MRI defecography are commonly used. These tests objectively demonstrate abnormal muscle activity during defecation and help distinguish anismus from structural bowel disorders.
How is anismus treated?
Treatment of anismus is mainly based on non-surgical approaches aimed at correcting abnormal muscle coordination. The cornerstone of therapy is pelvic floor rehabilitation and biofeedback therapy, which helps patients learn how to relax pelvic floor and anal muscles during defecation. Management also includes treating constipation, increasing dietary fiber intake, ensuring adequate fluid consumption, and improving bowel habits. In selected refractory cases, botulinum toxin (Botox) injections may be considered. Surgery is rarely indicated in the treatment of anismus.
What happens if anismus is left untreated?
If anismus is left untreated, symptoms usually worsen over time and chronic constipation may become persistent. Continuous straining leads to incomplete evacuation, increased bloating and gas, and prolonged time spent on the toilet. Long-term straining increases the risk of hemorrhoids, anal fissures, and pelvic floor weakness. Patients may also develop toilet-related anxiety, limitations in daily activities, and a significant decline in quality of life. Delayed treatment often results in a longer rehabilitation process and may require additional therapies.
Is anismus associated with other medical conditions?
Yes. Anismus often does not occur alone and may be associated with other anorectal and pelvic floor disorders. It is most commonly linked with chronic constipation. Prolonged straining may lead to hemorrhoids, anal fissures, and pelvic floor weakness. Some patients may also have rectocele, pelvic floor dysfunction, or functional bowel disorders such as irritable bowel syndrome (IBS). Therefore, evaluating coexisting conditions is essential for successful treatment.